Ultrasound for anti-incontinence surgery follow-up
In general, surgical complications are under-reported: only 2% of the articles published on monitoring surgical techniques meet all the quality criteria (6). Ultrasound can be extremely helpful in diagnosing and monitoring these situations.
In terms of time frame, we can divide these situations into perioperative complications (the most frequent is immediate postoperative voiding dysfunction), and long-term complications (such as lower urinary tract symptoms, also known as LUTS, pain, mesh erosion and stress incontinence recurrence.
Below we examine what ultrasound can contribute to the diagnosis and treatment of these situations.
Postoperative voiding dysfunction
A common occurrence after anti-incontinence surgery is the inability to completely empty the bladder, which can be attributed to two causes: detrusor atony (or hypocontractility) or urethral obstruction due to either compression on the pubis as proposed by Dietz (8) or to excessive urethral kinking as put forth by Sarlos (9). Ultrasound allows us to measure residual urine on the one hand, and, on the other hand, locate the mesh and evaluate whether it is obstructive.
a1. Residual urine test
The first step in diagnosing an obstruction is the evaluation of residual urine. Ultrasound allows us to perform this calculation non-invasively. Different authors have demonstrated the reliability of various formulas using either transperineal, vaginal or abdominal ultrasound (10,11,12).
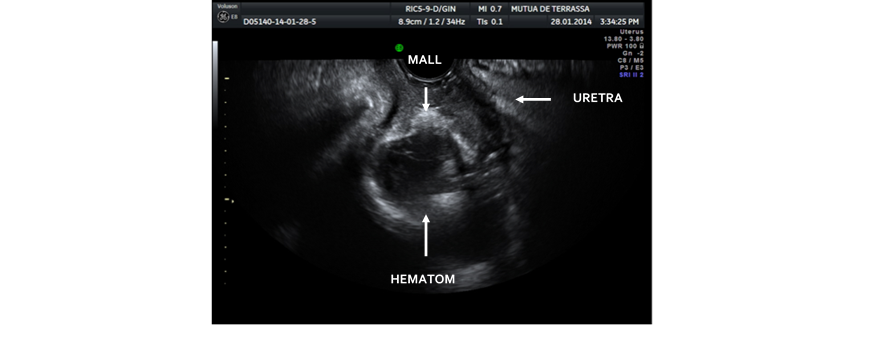
Once the obstruction is diagnosed, we must attempt to pinpoint its cause; as we've mentioned, the most frequent causes are bladder hypocontractility and obstruction due to mesh. Less frequently, the obstruction may be due to postoperative haematomas, which compress the urethra against the pubis. In these cases, the obstruction usually resolves itself when the haematoma is reabsorbed (Figure 1)
Figure 1. Postoperative haematoma that compresses the urethra, producing an infravesical obstruction
a2. Monitoring mesh implants
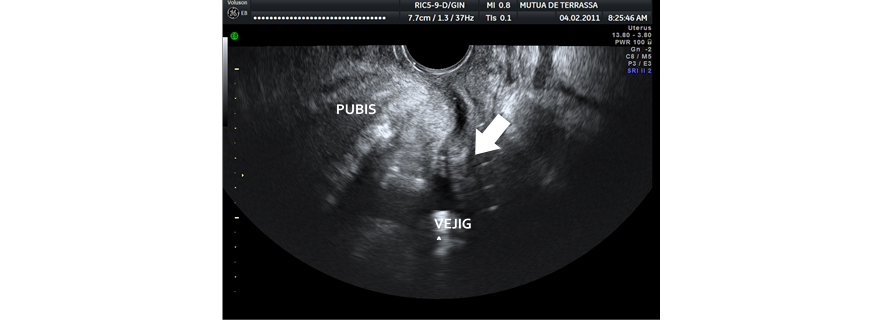
Ultrasound allows us to visualize the urethral trajectory and the anti-incontinence mesh. The urethral trajectory should be linear, without any curves; the italic S shape is typical when the mesh is excessively tense, directly correlating with obstruction (14) (Figure 2).
Figure 2. Italic S-shaped urethra; we can observe the compression of the urethra on the pubis
Chantarasorn correlated the mesh-pubis distance with obstruction (15). The position of the urethra is important, but so is its dynamic behaviour. Sarlos correlated an excessive kinking during the Valsalva manoeuvre with an increase in postoperative obstruction (9).
Kociszewski (16) correlated the shape of the mesh with the existence of tension: a flat mesh is not tense, but when the mesh adopts a C shape, it is. Visualization of the C-shaped mesh at rest is correlated with an increase of symptoms of obstruction.
In a more recent article, Kociszewski (17) also correlated obstruction with a proximal positioning of the mesh in relation to the urethral trajectory and with its location in relation to the urethral lumen (a mesh under 2mm away from the urethral sphincter will most likely be obstructive).
It is clear that there is no direct correlation between any ultrasonographic parameter and obstruction, but the coincidence between a high post-void residual and some of the ultrasonographic signs of obstruction lead us to consider a mechanical cause – excessive tension of the mesh – rather than a functional disorder.
Several authors have shown that in these cases, early intervention attempting to reduce tension on the mesh either by relaxing it surgically or by sectioning it (14) decreases obstruction and long-term irritative symptoms.
Ultrasonographic signs correlated with postoperative obstruction
Mesh in relation to urethral sphincter <2mm
Proximal mesh in relation to urethral length
C-shaped mesh at rest
Excessive urethral kinking at rest and with Valsalva
Decreased pubis-urethra distance
Italic S-shaped urethra
Complications in the mid and long term
Ultrasound can provide information on the mid and long-term complications associated with anti-incontinence mesh implants, as well as help us locate the mesh, allowing us to visualize its morphology and its relationship with different anatomical structures.
b1. Mesh erosion
The erosion rate of anti-incontinence mesh is around 2% (20), although this figure varies greatly depending on the case series and the type of mesh.
The mesh implants can erode into the vagina, bladder, urethra and perineal skin.
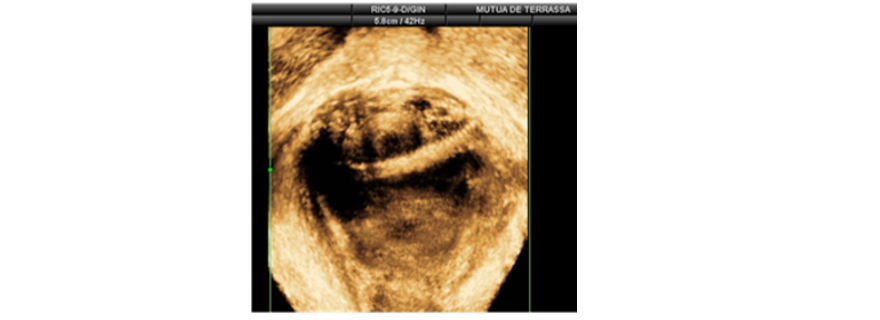
Ultrasound allows us to follow the trajectory of the mesh and its relationship with the different anatomical structures; it is relatively easy to visualize intraurethral (Figure 3)and intravesical mesh (21), especially with 3-D/4-D reconstruction. In cases of general vaginal erosion, the mesh is very far from the urethra and the vaginal wall.
Figure 3. Intraurethral mesh
We can observe abscesses or fistulous trajectories around the mesh when it presents with fistulisation that reaches the perineal skin. This information is valuable in cases of excision.
Ultrasound may also be useful intraoperatively, in order to locate mesh that we must be cut or removed (22).
b2. Pain
It is difficult to establish the incidence of postoperative pain with anti-incontinence mesh; depending on the case series, it varies between 0% and 30%. Pain may manifest as dyspareunia or inguinal pain - pain in the abductor area that occurs with movement.
The aetiology is not clear; some possibilities are mesh retraction, excessive tension, nerve or muscle injuries, or rubbing against the periosteum of the pelvis (23).
The ultrasound allows us to either directly or indirectly evaluate these circumstances. Asymmetric mesh with one band deeper in the obturator area can irritate the obturator nerve (Figure 4).
Figure 4. Asymmetric mesh in a patient who reports pain with movement
Mesh that is very close to the pubic periosteum or the ischiopubic ramus can irritate the area, thus producing pain. Mesh that overcorrects the urethra may present with retraction or excessive tension.
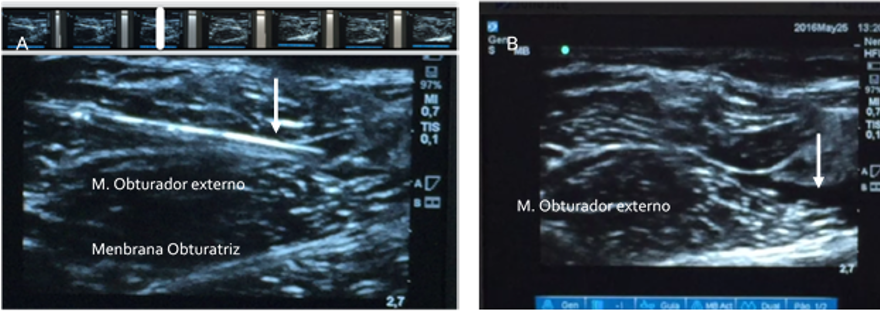
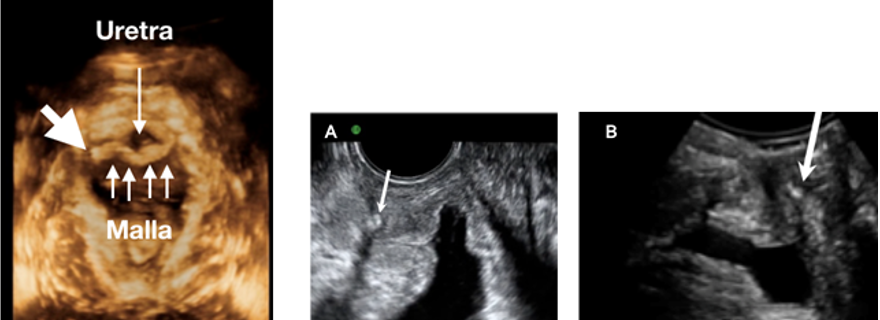
The ultrasound also allows for infiltrations with local anesthetics +/- corticosteroids to try to reduce the retraction or perform nerve blocks if obturator nerve involvement is suspected (Figure 5).
Figure 5. Anaesthetic obturator nerve block. A - Path of the needle (arrow) over the external obturator muscle. B - Anaesthetic weal (indicated by arrow) at the obturator membrane nerve root
If this first approach does not solve the problem, the use of intra-operative ultrasound facilitates the location of the mesh for its complete removal (22).
When mesh removal is necessary due to pain, the pain disappears completely in 81% of patients (23).
b3. Lower urinary tract symptoms (LUTS)
The most frequent complications after the placement of an anti-incontinence mesh tend to be voiding dysfunctions, with an incidence of 1-10% and de novo urgency that affect 6-10% of patients. These two entities are intimately correlated: some cases of de novo urgency are secondary conditions due to obstruction (24).
The obstruction is also correlated with some cases of recurrent lower tract infections. Different authors have correlated the ultrasonographic appearance of mesh – its positioning in relation to urethral length and urethral lumen – with obstruction and urge incontinence.
Kociszewski (16, 17) assessed several static ultrasonographic parameters, (position of the mesh in relation to the urethra) and dynamic parameters (change of the mesh shape during the Valsalva manoeuvre) in relation to postoperative complications. There is a direct correlation between the irritative symptoms of voiding and urge incontinence, with a position of the mesh under 3 mm away from the sphincter complex.
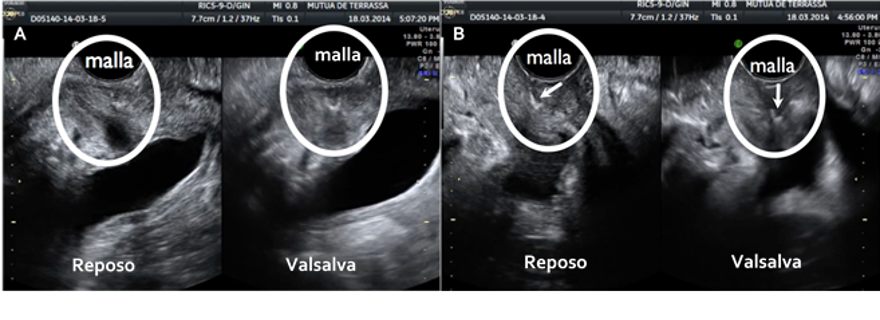
The dynamic response of the mesh is also important: tension-free mesh is visualized as flat, while it takes on a C shape when it is tense. The ideal situation would be to visualize the mesh as flat and tension-free at rest, and in a C shape when performing the Valsalva manoeuvre, compressing the urethra (Figure 6).
Figure 6. A - Ideal visualization of the mesh: flat at rest, C-shaped with Valsalva. B- Excessively tense C-shaped mesh at rest and with Valsalva manoeuvre
When the mesh is C-shaped at rest, it indicates that it is too tight, which in some cases results in obstruction.
Therefore, if we observe a mesh that is fewer than 3 mm from the urethral lumen or that is C-shaped at rest in a patient with obstruction, signs and symptoms of urgency or recurrent urinary tract infections, we can consider the possibility of sectioning the mesh in order to release tension (14). In these cases, the symptoms of obstruction and urgency disappear in 89% of patients after the mesh has been sectioned (Figure 7).
Figure 7. 3-D view of sectioned mesh (on the right). Image in 2-D. A- Mesh before section, in a C shape and obstructing the urethra. B- Flat post-section mesh at rest
b4. Recurrence of incontinence
Recurrent incontinence, a very unpleasant situation both for the patient and surgeon, is when a patient continues to report stress incontinence after undergoing anti-incontinence surgery.
Ultrasound is very useful in these cases. From the outset, we can easily rule out an obstructed patient with overflow incontinence.
Different authors (17, 25, 26) have related surgical errors with three factors related to the position and dynamic behaviour of the mesh.
1. Position in relation to total urethral length (in %).
The persistence of stress incontinence is more frequent in patients with mesh placed in the proximal third of the urethra, near the bladder neck, or between the proximal and medial third (26), due to the impossibility of urethral kinking. The ideal placement for obtaining continence is at between 50 and 80% of the urethral length.
2. Position in relation to the urethral sphincter complex.
Another fundamental factor is the distance of the mesh from the sphincter complex: when the mesh is > 5 mm from the sphincter complex, the relative risk for the patient remaining incontinent is 5.2 times greater (16).
3. Dynamic behaviour during the Valsalva manoeuvre.
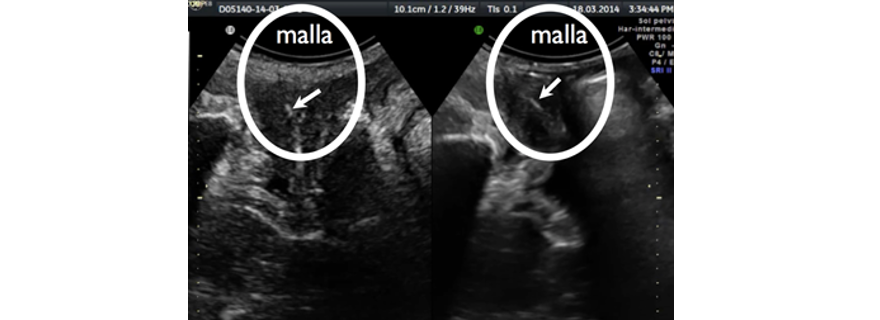
In patients who continue to suffer from incontinence after surgery, we are more likely to visualize the mesh as flat during the Valsalva manoeuvre, which indicates that the urethra is not resting on the mesh and that kinking cannot occur (Figure 8).
Figure 8. Mesh at rest / Valsalva without changes in a patient with postoperative incontinence
Other authors, such as Hedge (25), correlate continence with the concordance of the movement of the mesh and the urethra during the Valsalva manoeuvre; this means that the urethra is immobile or that the mesh is very far from it.
Other authors (27) have correlated the decrease in the urethral core, the hypoechogenic part of the urethra, with continence after surgery. In patients who continue to experience incontinence, there is no decrease in the core due to lack of support or "kinking" of the urethra on the mesh.
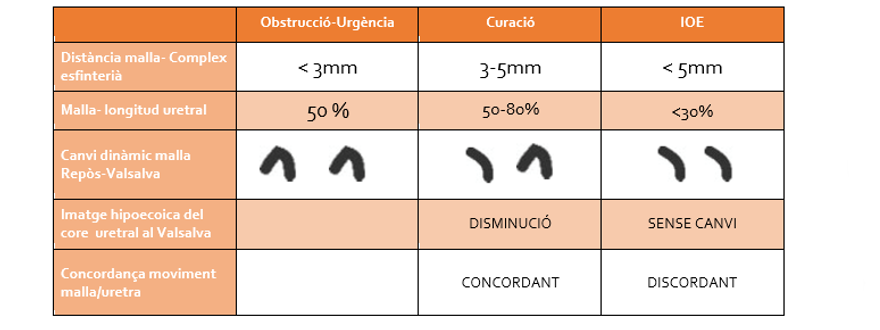
The ultrasonographic findings that correlate with different outcomes after surgery with tension-free mesh are summarized in Table 1.
TABLE 1.Summary of ultrasonographic findings that correlate with postoperative intcontinence outcomes