Pelvic floor ultrasound may be useful for various aspects of managing pelvic organ prolapse, including:
Pre-surgically selecting patients with higher risk of recurrence and patients with levator ani injury or with a large urogenital hiatus
Postoperatively assessing and managing complications associated with prolapse surgery as well as assessing cases of recurrence
In terms of research, studying the behaviour of the mesh net in order to improve its design and development
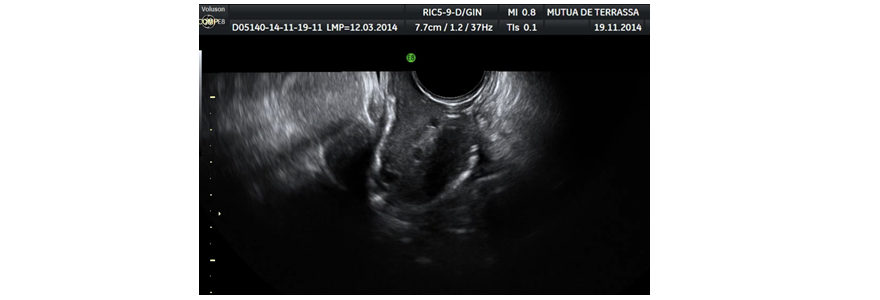
It seems that the levator ani injury is one of the biggest risk factors for the development of genital prolapse. Different authors have correlated certain ultrasonographic findings with an increased rate of recurrence after prolapse surgery. Dietz (28) and Volløyhaug (29) demonstrated the impact of levator ani injury (Figure 9) and ballooning (20) years after delivery. This serves to confirm DeLancey's biomechanical theory (30) that the triggering factor of apical and anterior prolapse is injury to the levator ani muscle.
Figure 9. Avulsion of the right levator ani in TUI (tomographic ultrasound imaging)
In addition, it appears that levator ani injury is an important prognostic factor in the rate of recurrence after genital prolapse surgery; Dietz (31) and Weenhoff (32) correlated avulsion with postoperative cystocele recurrence, while Model (33) correlated it with recurrence after prolapse surgery in general.
In a recent meta-analysis, Friedman (34) found that the most important risk factor for postoperative recurrence of genital prolapse is the levator ani avulsion, followed by the degree of prolapse and family history.
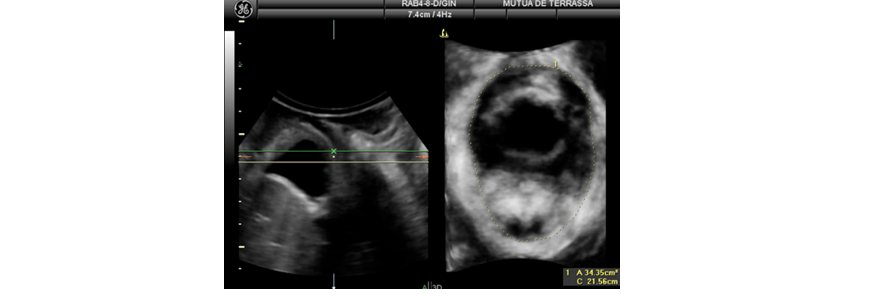
It also seems that hiatal ballooning, the distension of the levator ani muscle that increases the area of the hiatus during the Valsalva manoeuvre, is an independent factor both for the onset of prolapse and for its postoperative recurrence (35, 36) (Figure 10).
Figure 10. Area of hiatus during the Valsalva manoeuvre in a patient with ballooning. The dotted line shows the rendered image
Wong (37) showed that levator ani muscle injury exacerbates outcomes in patients operated on with vaginal mesh for prolapse.
Currently, many groups are considering whether ultrasonographic indicators of risk of recurrence, such as avulsion and ballooning, should modify the surgical technique implemented in order to reduce the rate of recurrence.
One of the most difficult complications when using vaginal mesh is the contraction/retraction of the material from which a series of conditions may ensue, including vaginal pain aggravated by movement, dyspareunia, thickening of the vaginal wall with sensitivity to touch and vaginal shortening (38).
Rogowsky (39) also correlated mesh retraction measured by ultrasound with the intensity of pain and the emergence of overactive bladder. Ultrasound helps provide evidence of this retraction; Tunner (40) demonstrated an almost 60% reduction of the mesh area just months after its placement.
The debate centers on whether this retraction is due to excessive fibrosis during the healing process or to technical aspects of the mesh placement. Shabik (41) demonstrated that the decrease in mesh size is mainly due to intraoperative wrinkling and depends more on the placement technique than on subsequent behaviour. In a study of 60 patients, Dietz (42) failed to demonstrate ultrasonographic evidence of retraction; what's more, he observed an increase in mesh length over time, which may point to long-term collagen remodelling.
It is clear that ultrasound allows us to provide evidence of mesh retraction or wrinkling in symptomatic patients. There is a good correlation between the ultrasonographic thickness of the mesh, the hyper-refraction and retraction (43).
Another important area of ultrasound application is in the evaluation of patients that have experienced recurrence after mesh or classic surgery. The group led by Jacquet correlated ultrasonographic findings in cases of recurrence after total proliferation that is associated with severe mesh retraction or loss of support in the distal vaginal wall (43). In a long series of ultrasonographic tests of various types of mesh, Shek (44) managed to sort the types of failures as follows: 3% caudal failures when the distal anchors fail, 8% apical failures when the upper support fails and 27 % global failures when all four anchors fail.
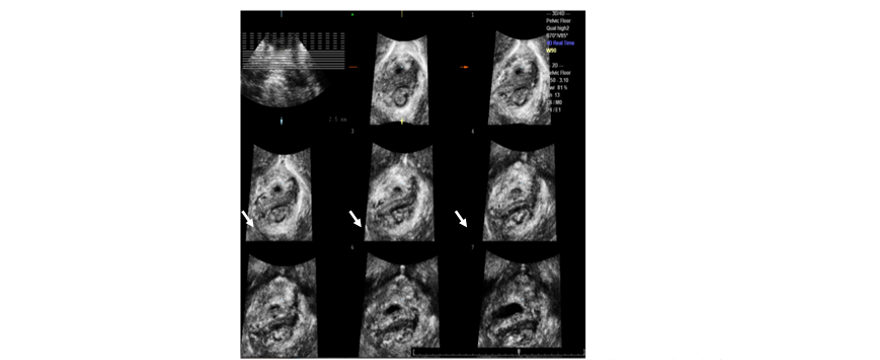
Other authors such as Eisenberg (45, 46) and Wong (47) studied the role of ultrasound in the monitoring of mesh implants using laparoscopic colposacropexy. Eisenberg demonstrated a good visualization of the anterior and posterior mesh, as well as the convergence point in practically all the patients, while it is much more difficult to visualize the commonly used mesh that is fixed to the sacrum (Figure 11).
Figure 11. Visualization of anterior mesh (long arrows) and posterior mesh (short arrows) in colposacropexy
Wong demonstrated that recurrence in the anterior face with the emergence of a symptomatic cystocele is directly correlated with a decrease in the caudal positioning of the anterior mesh.
In cases of apical recurrence when a hysteropexy has been performed, ultrasound is very useful for evaluating whether it is a real recurrence or a cervical elongation, the latter of which is a common complication in this type of surgery (48). In the first case, if the recurrence is caused by tearing from the sacrum, we can re-anchor the mesh, while if what we have is a cervical elongation, a trachelectomy will suffice to solve the problem.