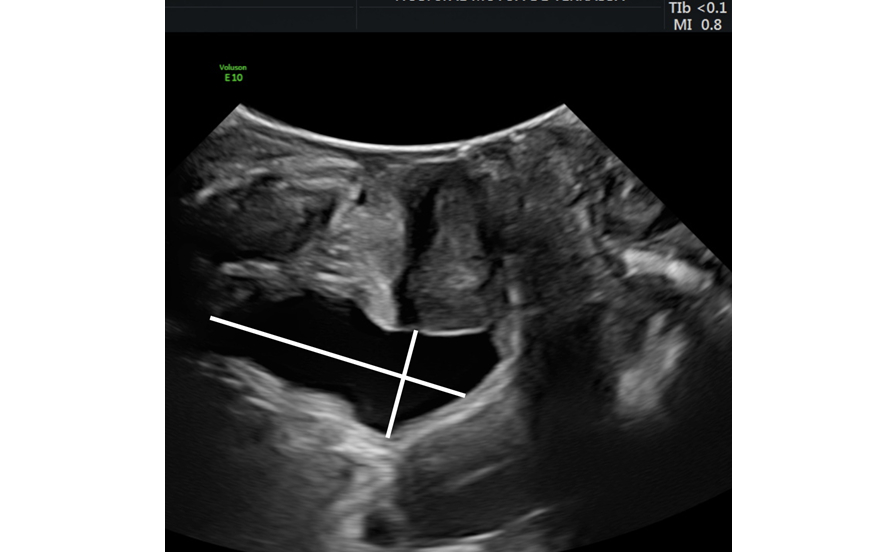
The use of ultrasound in studying incontinence begins with the assessment of the residual urine test. Testing residual urine is important in order to rule out a voiding dysfunction. In 1989, Haylen assessed the accuracy of ultrasound in measuring the volume of residual urine in operated patients (1). He compared the volume obtained by ultrasound to that obtained by bladder catheterization and saw that there was a very good correlation between the two, especially between 50 and 200 ml. There are numerous formulas to assess the volume of residual urine. Haylen's proposal consists of A ×B × 5.9 - 14.6, where A and B are the anechogenic part of the bladder contents in depth and height, measured in the sagittal plane (1) (Figure 5). Other formulas use the transverse plane, measuring the anechogenic part of the bladder contents in a transversal slice, as is the case with Dicuio's formula. Still other formulas, such as that proposed by Dietz, only use the sagittal plane and a single conversion factor: X × Y × 5.6, where X and Y are the height and depth of the bladder contents (3) (Figure 5). It is also possible to assess the residual volume by means of three-dimensional ultrasound with a portable ultrasound scanner (bladder scanner), or with a specific software program installed in the ultrasound machine has (for example, the GE VOCAL program).
Figure 5. Measurement of residual volume using the maximum depth and height of anechogenic bladder content
It is difficult to assess voiding dysfunction based solely on clinical manifestation. Sometimes it presents as strangury or difficulty with urination, but this is not always the case; sometimes its clinical expression may seem to indicate stress urinary incontinence or signs and symptoms of urgency.
It is important to assess voiding dysfunction in operated patients; it is often associated with uterine prolapse. If we do not take notice and do not consider the possibility of voiding dysfunction, over time it could trigger ureterohydronephrosis, resulting in possible renal failure. Bladder diverticulum can also appear in the case of a bladder that is struggling to overcome an obstruction, or from another, more frequent, pathology such as repeated urinary tract infections.
It therefore no longer makes sense to perform a catheterization (which is clearly a gruelling procedure) in order to assess post-void residual, when it can be assessed just as well by ultrasound.