There are two types of stress urinary incontinence: one that is caused by excessive mobility of the urethra (urethral hypermobility) and one which occurs due to a sphincter deficiency. Seeing that both are anatomical dysfunctions in which anatomical changes have taken place, an ultrasound can probably provide us with useful findings.
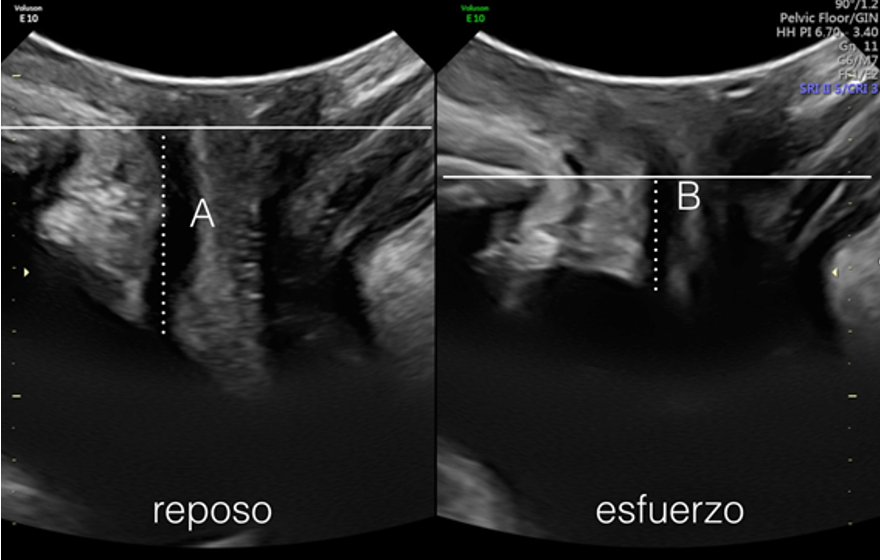
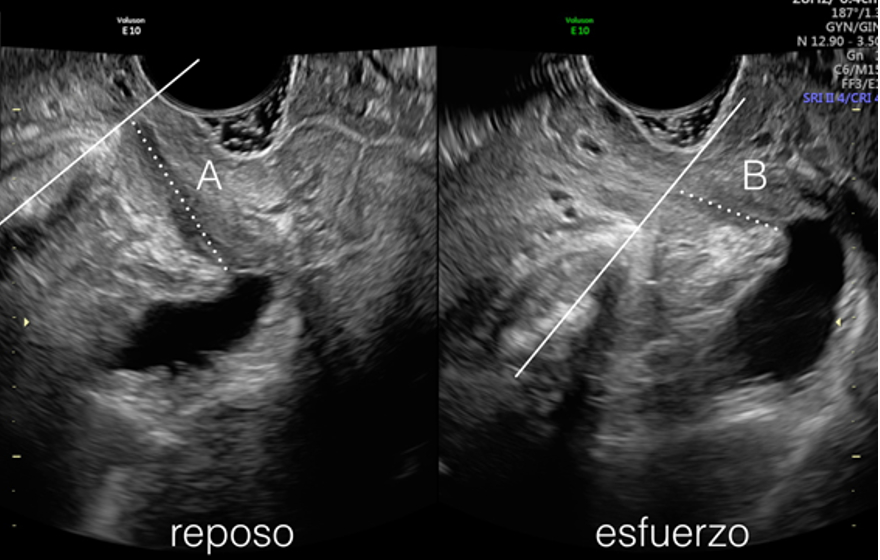
Different ways of measuring urethral hypermobility have been outlined, including using urethral sliding, the rotation angle, the assessment of the retrovesical angle, etc. Mobility is usually measured from a fixed plane, which can be horizontal with the symphysis (4) (Figure 6 and Clip 2) where from the symphysis axis (5) (Figure 7). There is no cut-off point at which patients cease to be continent and become incontinent, since incontinence does not depend solely on one parameter, such as hypermobility, but instead depends on additional factors, such as sphincter function and other parameters. We can therefore see patients with mobile urethras who are perfectly continent.
Figure 6. The continuous line marks the horizontal axis in relation to the pubis; the dotted line indicates the mobility of the urethra, which is obtained from the difference between A and B (rest and stress).
Figure 7. The continuous line marks the axis of the pubis; the dotted line indicates the mobility of the urethra, which is obtained from the difference between A and B (rest and exertion)
Another limitation when establishing base-line normal data is that during the performance of the Valsalva manoeuvre, patients may be simultaneously contracting their pelvic musculature for fear of urine leakage.
The assessment of the urethral sphincter has also been studied ultrasonographically with a good intra and interobserver correlation when using three-dimensional ultrasound. It has been observed that among incontinent patients who have undergone Burch colposuspension, those who continued to be incontinent had smaller ultrasonographic sphincter volumes than those who were cured. This points to an anatomical translation of a functional problem; however, sphincter changes and the proper function of the urethral sphincter are, without a doubt, better assessed using urodynamics instead of ultrasound.
In a recent study conducted at our centre, we saw that both urethral mobility and length at rest were the best markers of stress urinary incontinence. Thus, with a cut-off point of 3.5 cm or shorter for urethral length, we obtained a sensitivity of 81.5% and a specificity of 43.6% for the diagnosis of stress incontinence. Patients with urethral mobility above 18 mm were more associated with stress incontinence, with a sensitivity of 67% and a specificity of 74%. Therefore, the role of urethral and sphincter mobility in urinary continence is important, although it is impossible to obtain cut-off points with 100% sensitivity and specificity, given that other factors are involved.
Another important aspect is the opening or funnelling of the bladder neck (Clip 3). This is usually associated with sphincter deficiency, but it can also be due to an overactive detrusor, which triggers uninhibited contraction, thus causing the bladder neck to open.
In one prospective study, patients without previous funnelling had a better outcome after surgery than those who had previous funnelling; it is therefore a prognostic factor. It also has a very high negative predictive value: 92.8% as a marker of sphincter pressure (7).
In relapsed or irradiated patients, the therapeutic decision is conditioned by the prior assessment of whether or not there is urethral mobility, which is where the ultrasound proves to be very useful. In an immobile urethra, tension-free mesh will not solve the problem.
It's important to try to avoid false images when assessing funnelling, as the condition could be confused with a cystocele.